



Juvenile Papillomatosis (Swiss Cheese Disease) of the Breast
- László Tabár, MD and Kevin M. Rice, MD
- Dec 6, 2015
- 5 min read
Updated: Mar 11, 2021
Right Breast Mass in 24F • Xray of the Week 2017 • Week #6

This 24 year old woman presented with a self-detected hard mass in the upper inner quadrant of her right breast. Her paternal grandmother had breast cancer at age 34 and died of the disease at age 54. Clinical breast examination confirmed the presence of a freely mobile hard tumor with irregular borders. No skin changes or discharge were present. The axillary lymph nodes were normal by palpation. What unusual type of breast mass could this be in this young lady?

Figure 1. Bilateral mammogram shows a high density mass with indistinct margins in the right breast centrally. The metal BB marker indicates it is palpable. The left breast is normal.

Figure 2. Left image: MLO mammogram shows a high density mass with indistinct margins in the right breast centrally. The metal BB marker indicates it is palpable.
Right image: Magnification mammogram shows the mass with indistinct margins and associated grouped fine pleomorphic microcalcifications and possible spiculation.

Figure 3: Ultrasound images show a hypoechoic right breast nodule with distended ducts, some of which having cystic dilatation.

Figure 4: A,B. Axial MRI with contrast images show bilateral considerable background contrast enhancement. Left breast: normal MRI finding. Right breast: 4 cm deep to the nipple at 2:00, there is a 2.2 x 1.8 cm triangle shaped heterogeneous non-mass enhancement, suspicious for in situ or/and small invasive cancer focus. C,D. Sagittal MRI with contrast. No pathologic lymph nodes are seen in the axilla. MRI images courtesy of Andreas Adam, MD

Figure 5: Ultrasound images show biopsy of the mass. Histology was hyperplastic breast change, most probably Juvenile Papillomatosis (Swiss Cheese Disease) of the Breast. No signs of malignancy.
Due to the suspicious appearance on mammography and MRI, ultrasound biopsy was performed [Fig.5] followed by excision of the mass. Pathology was juvenile papillomatosis (Swiss cheese disease) of the breast.

Figure 6: Specimen radiograph of excisional biopsy with associated large section histology. There is no invasive component. Histology images are courtesy of Tibor Tot, MD PhD - Associate Professor, Department of Pathology and Clinical Cytology, Central Hospital Falun, Falun, Sweden.
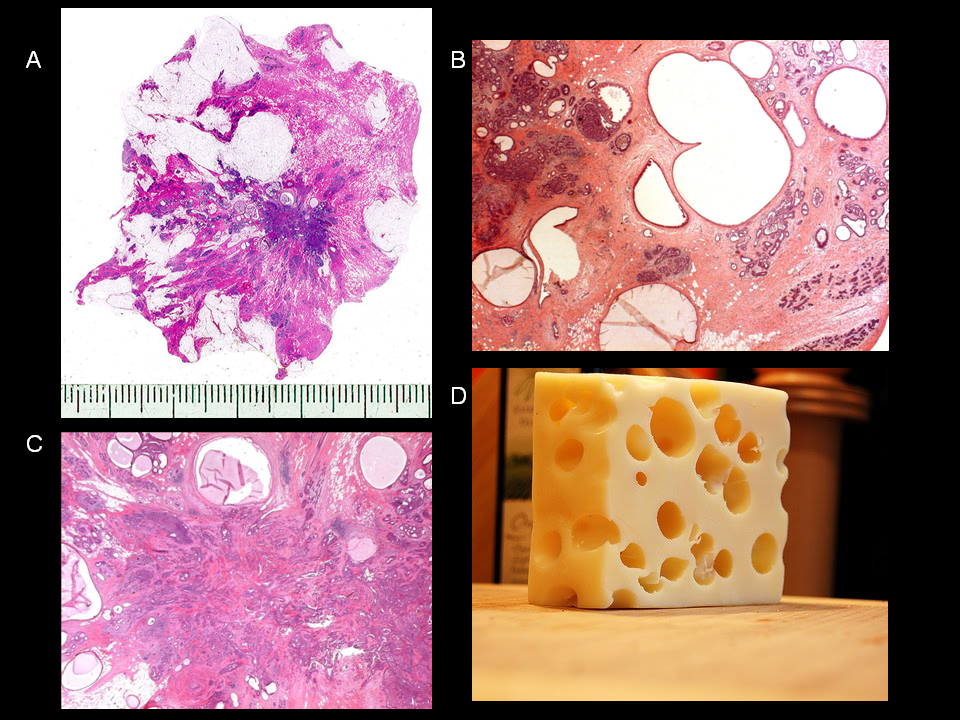
Figure 7: A. Histology demonstrated a 25 x 20 mm mass with the appearance of Swiss cheese disease (Juvenile papillomatosis). B. Multiple benign cysts within the stroma. C. Multiple benign papillomas with florid epithelial hyperplasia. A central papilloma with sclerotic stroma gives the impression of a stellate mass; however, there is no histologic evidence of malignancy. D. Actual Swiss cheese. Histology images are courtesy of Tibor Tot, MD PhD - Associate Professor, Department of Pathology and Clinical Cytology, Central Hospital Falun, Falun, Sweden
Discussion
Juvenile papillomatosis is a rare benign proliferative breast process which occurs in women with a mean age of 19-23 and is rare over age 40 [1-6]. On histology the lesion demonstrates papillary epithelial hyperplasia within the small ducts and lobules [1-9]. Numerous cysts and dilated ducts are present, separated by areas of dense stroma, which results in the characteristic “Swiss cheese” appearance [9] [Figs. 6-7]. Juvenile papillomatosis occasionally may be associated with severe atypia or focal epithelial necrosis, features which are considered pre-malignant in older women [9]. Clinically, juvenile papillomatosis has benign findings with a firm, mobile well-circumscribed mass in a young patient. As in this case, mammography may demonstrate a spiculated mass with microcalcifications [Figs. 1-2]. Ultrasound typically shows a heterogeneous mass with small cystic regions, which correspond to the small cysts seen histologically [8-10] [Figs. 3,5]. According to a case report, MRI demonstrated a lobulated mass which was low in signal intensity on T1-weighted images and showed marked contrast enhancement. In the dynamic sequence the lesion showed a benign enhancement profile. Multiple small internal cysts were best shown on the T2 weighted images [3] [Fig. 4]. As with the patient in this case, juvenile papillomatosis is a marker for familial breast cancer. Moreover, patients diagnosed with the disease are at higher risk for breast cancer, especially if there is bilateral or recurrent juvenile papillomatosis or there is a family history of breast cancer [8]. Treatment is wide surgical excision [Figs. 8-10].
In cases such as this, the radiologist plays a very important role in the workup and diagnosis. During the evaluation of this 24 year old patient, Dr. Tabár emphasized that although there was a suspicious enhancement pattern on MRI, the ultrasound demonstrated very benign features with small cysts and dilated ducts and no malignant features whatsoever. Since juvenile papillomatosis represents actively proliferating hyperplastic breast epithelial tissue, it is not surprising to find that it enhances on MRI. A malignant breast tumor would not have cystic changes and proliferating ducts within the tumor on ultrasound. There are 2 types of hyperplastic breast change that would have this ultrasound appearance- radial scar which is usually not palpable, and juvenile papillomatosis (Swiss cheese disease) which is palpable in most cases.
Other breast imaging cases on Global Radiology CME:
References:
1. Kaneda HJ, Mack J, Kasales CJ, et al. Pediatric and Adolescent Breast Masses: A Review of Pathophysiology, Imaging, Diagnosis, and Treatment. American Journal of Roentgenology. 2013;200: W204-W212.
2 Batori M, Gallinaro LS, D'urso A et-al. Papillomatosis and breast cancer: a case report and a review of the literature. Eur Rev Med Pharmacol Sci. 4 (4): 99-103.
3. Mussurakis S, Carleton PJ, Turnbull LW. Case report: MR imaging of juvenile papillomatosis of the breast. Br J Radiol. 1996;69 (825): 867-70.
4. Chung EM, Cube R, Hall GJ et-al. From the archives of the AFIP: breast masses in children and adolescents: radiologic-pathologic correlation. Radiographics. 29 (3): 907-31.
5. Sabate JM, Clotet M, Torrubia S et-al. Radiologic evaluation of breast disorders related to pregnancy and lactation. Radiographics. 2007;27 Suppl 1 : S101-24.
6. Kersschot EA, Hermans ME, Pauwels C et-al. Juvenile papillomatosis of the breast: sonographic appearance. Radiology. 1988;169 (3): 631-3.
7. Rosen PP, Cantrell B, Mullen DL et-al. Juvenile papillomatosis (Swiss cheese disease) of the breast. Am. J. Surg. Pathol. 1980;4 (1): 3-12.
8. Rosen PP, Holmes G, Lesser ML et-al. Juvenile papillomatosis and breast carcinoma. Cancer. 1985;55 (6): 1345-52.
9. Rosen PP, Kimmel M. Juvenile papillomatosis of the breast. A follow-up study of 41 patients having biopsies before 1979. Am. J. Clin. Pathol. 1990;93 (5): 599-603.
10. Al sarakbi W, Worku D, Escobar PF et-al. Breast papillomas: current management with a focus on a new diagnostic and therapeutic modality. Int Semin Surg Oncol. 2006;3 : 1

László Tabár, MD, FACR (Hon) the Professor Emeritus of Radiology Uppsala University, Faculty of Medicine, Sweden and the Medical Director Emeritus of the Department of Mammography, Falun Central Hospital, Sweden. Through his company, Mammography Education, Inc, he has also been the course director and principal lecturer at more than 300 mammography courses on 6 continents. His pioneering research has laid the foundation for early detection through modern mammographic screening. Dr. Tabár is the recipient of numerous awards including the Gold Medal from the Society of Breast Imaging, American Cancer Society's Distinguished Service Award, and the first Alexander Margulis Award for Scientific Excellence from the Radiological Society of North America (RSNA). Dr. Tabár will be sharing his vast knowledge of breast imaging at Imaging in Israel - 2017.

Kevin M. Rice, MD is the President of Global Radiology CME
Dr. Rice serves as the Chair of the Radiology Department of Valley Presbyterian Hospital in Los Angeles, California and is a radiologist with Renaissance Imaging Medical Associates. Dr. Rice has made several media appearances and as part of his ongoing commitment to public education. Dr. Rice's passion for state of the art radiology and teaching includes acting as a guest lecturer at UCLA. In 2015 Dr. Rice founded Global Radiology CME to provide innovative radiology education at exciting international destinations, with the world's foremost authorities in their field. In 2016, Dr. Rice was nominated and became a semifinalist for a "Minnie" award for the Most Effective Radiology Educator.
Follow Dr. Rice on Twitter @KevinRiceMD














Comments