



Stanford B Aortic Dissection
- Han Ngo and Kevin M. Rice, MD
- Jul 27, 2020
- 5 min read
Updated: Feb 26, 2024
58 yo Male Chest pain. Abdominal and pelvic pain radiating to the back. Hypertension • Xray of the Week
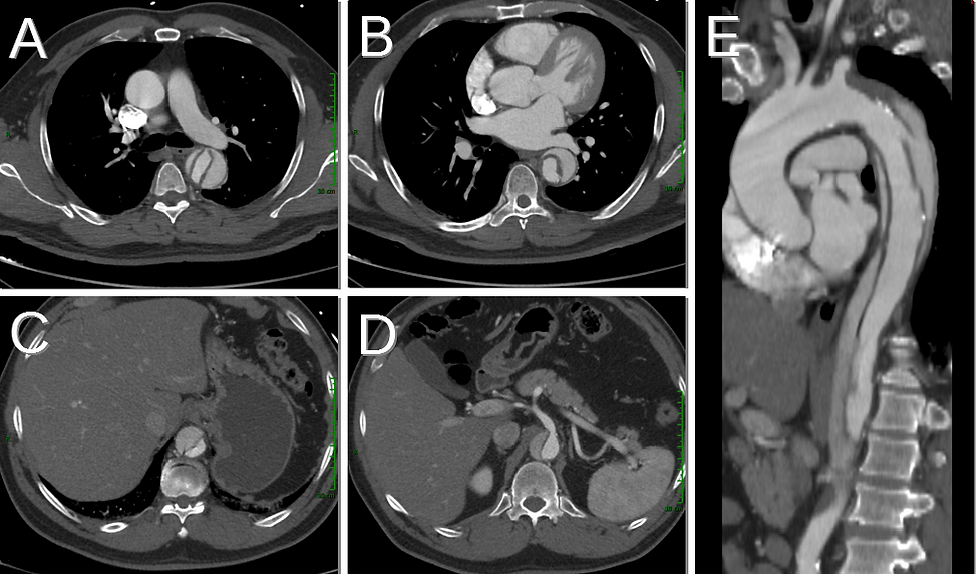
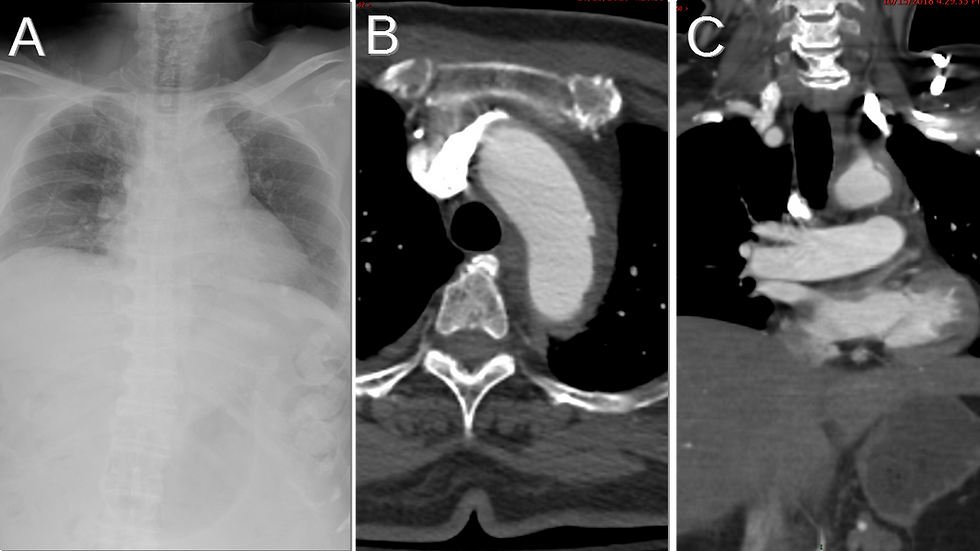
Figure 1. Name the important findings on this CT Scan.

Figure 2. Stanford Type B aortic dissection. On chest CT, red arrows point at the true aortic lumen and yellow arrows point at the false aortic lumen at the levels:
A- Mid ascending aorta
B- Aortic root
C- Upper abdomen
D- Celiac axis
E- Delineates the extent of dissection in the descending aorta. Intimal flap is the low attenuation linear region between the true and false lumen.

Figure 3. Diagram showing a cross section of the aorta at the level of aortic dissection. A tear in the aortic intima leads to blood leaking from the true aortic lumen into the false lumen. The two lumens are separated by an intimal flap, the key diagnostic finding of aortic dissection on imaging. Diagram by Han Ngo.

Figure 4: Diagram of Stanford classification for aortic dissection. Stanford Type A involves the ascending aorta with or without descending aortic involvement. Stanford Type B involves the descending aorta distal to the left subclavian artery. Intimal flap is the piece of teared intima that separates the true aortic lumen from false aortic lumen. Diagram by Han Ngo.
Discussion:
Aortic dissection occurs when there is a tear in the intima of the aortic wall, resulting in blood leaking from the true lumen into the media. The blood that travels to the media creates a false lumen, which is separated from the true lumen by a layer of defective intima called intimal flap (1) (Figure 3). Aortic dissection is most commonly seen in elderly patients with systemic hypertension. Connective tissue disorders (e.g. Marfan’s syndrome, Ehlers-Danlos syndrome), bicuspid aortic valve, aortic coarctation, smoking, hyperlipidemia, cocaine use, deceleration trauma, and iatrogenic injury are other risk factors that have been associated with aortic dissection (2,3).
Patients with aortic dissection often present with sudden onset of severe chest pain, typically described as “sharp” or “tearing” in sensation. Depending on the location of aortic dissection, patients may also present with a blood pressure difference between the two arms (4,5). Other symptoms such as abdominal pain, syncope, stroke, or acute renal failure may also result due to decreased blood supply to organs (2-4). If left untreated, aortic dissection can be fatal within the first 24-48 hours due to aortic rupture or insufficient blood flow to the heart (6).
Aortic dissection can be categorized by the Stanford classification system (Figure 4). In Stanford Type A, aortic dissection occurs at the level of the ascending aorta, with or without descending aortic involvement. In Stanford Type B, aortic dissection affects the descending aorta distal to the left subclavian artery. Usually, Stanford Type A is treated surgically or with stent-graft placement while Stanford Type B is managed medically, primarily with blood pressure control (3-7).
Medical imaging is imperative for the diagnosis of aortic dissection and for the Stanford classification (which guides the disease treatment). Common imaging modalities currently used to confirm aortic dissection include CT, transesophageal echocardiography, and MRI with CT being the most common due to its wide availability, high accuracy, and ability to produce images rapidly. The key diagnostic finding on chest CT and MRI is the presence of an intimal flap separating the true and false aortic lumens. The two lumens can be distinguished based on size and contrast density: the false lumen is often larger and has lower contrast density than the true lumen (2,3,8) (Figures 1,2).
In summary, the key to successful management of aortic dissection requires early clinical suspicion followed by correct choice of imaging tests to confirm the diagnosis and prompt initiation of treatment based on the Stanford classification system. Since the highest risk for complications (e.g. aneurysm, recurrent dissection) occurs in the first two years after the initial presentation, patients with aortic dissection should be followed up closely with CT or MRI imaging of the aorta at 1, 3, 6, and 12 months and then annually over the long term (6,7).

References:
1. Juang D, Braverman AC, Eagle K. Aortic dissection. Circulation. 2008;118(14). doi:10.1161/CIRCULATIONAHA.108.7999082
2. Alfson DB, Ham SW. Type B Aortic Dissections: Current Guidelines for Treatment. Cardiol Clin. 2017;35(3):387-410. doi:10.1016/j.ccl.2017.03.0073
3. Kamalakannan D, Rosman HS, Eagle KA. Acute aortic dissection. Crit Care Clin. 2007;23(4):779-vi. doi:10.1016/j.ccc.2007.07.0024
4. Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897-903. doi:10.1001/jama.283.7.8975
5. Salameh MJ, Ratchford E V. Aortic dissection. Vasc Med. 2016;21(3):276-280. doi:10.1177/1358863X166328986
6. Juang D, Braverman AC, Eagle K. Aortic dissection. Circulation. 2008;118(14). doi:10.1161/CIRCULATIONAHA.108.7999087
7. Hiratzka LF, Bakris GL, Beckman JA et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: executive summary. J Am Coll Cardiol 2010;55(14):1509–1544. doi:10.1016/j.jacc.2010.02.0108
8. Nienaber CA, Clough RE. Management of acute aortic dissection. Lancet. 2015;385(9970):800-811. doi:10.1016/S0140-6736(14)61005-9

Han Ngo is a medical student at Oakland University William Beaumont School of Medicine (OUWB) in Rochester, Michigan. She graduated from UCLA, receiving her B.S. degree in Biochemistry. Prior to starting medical school, Han spent 4+ years (including her undergraduate years) working as a medical scribe for a psychiatrist at Ronald Reagan UCLA Medical Center. Interested in radiology, Han is now serving as the President of both diagnostic radiology and interventional radiology interest groups at OUWB. She is also a committee member on the Medical Student Council of the Society of Interventional Radiology (SIR). After deciding on her specialty, Han plans to continue learning and striving to make a difference in patients’ lives.
Follow Han Ngo on Twitter @Han_Ngoo

Kevin M. Rice, MD is the president of Global Radiology CME and is a radiologist with Cape Radiology Group. He has held several leadership positions including Board Member and Chief of Staff at Valley Presbyterian Hospital in Los Angeles, California. Dr. Rice has made several media appearances as part of his ongoing commitment to public education. Dr. Rice's passion for state of the art radiology and teaching includes acting as a guest lecturer at UCLA. In 2015, Dr. Rice and Natalie Rice founded Global Radiology CME to provide innovative radiology education at exciting international destinations, with the world's foremost authorities in their field. In 2016, Dr. Rice was nominated and became a semifinalist for a "Minnie" Award for the Most Effective Radiology Educator. He was once again a semifinalist for a "Minnie" for 2021's Most Effective Radiology Educator by AuntMinnie.com. He has continued to teach by mentoring medical students interested in radiology. Everyone who he has mentored has been accepted into top programs across the country including Harvard, UC San Diego, Northwestern, Vanderbilt, and Thomas Jefferson.
Follow Dr. Rice on Twitter @KevinRiceMD













Comments